

Introduction:
Daratumumab (Dara) is a human anti-CD38 monoclonal antibody approved for multiple myeloma (MM) treatment. Dara has shown promising efficacy and a favorable safety profile in newly diagnosed (ND) and relapsed refractory MM patients. This study is focused on the efficacy and safety of Dara when added to the standard care regimen in transplant eligible newly diagnosed MM (NDMM) in phase III clinical trials.
Methods:
We performed a comprehensive literature search on four databases (PubMed, Embase, Cochrane, and Clinicaltrials.gov). Our search strategy included MeSH (Medical Subject Headings) terms and keywords for multiple myeloma and Dara including trade names and generic names from date of inception to May 2020. Initial search revealed 588 articles. After a detailed screening, two phase III randomized clinical trials were included, which reported overall response rate (ORR) and negative minimal residual disease (MRD) in transplant eligible MM patients with Dara addition to standard care regimen. Odds ratios (OR) of ORR and MRD were computed along with 95% confidence intervals (CI) for pooled analysis using a fixed-effect model in RevMan v.5.4.
Results:
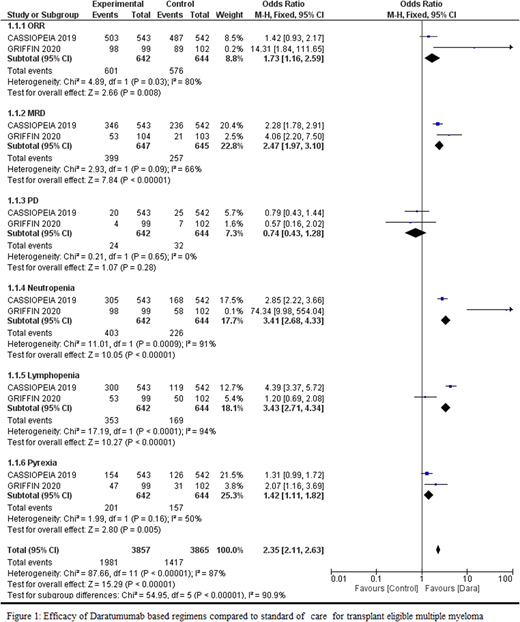
A total of 1292 transplant eligible NDMM patients were enrolled and evaluated in two phase III randomized controlled trials. Six hundred and forty-seven patients were in the Dara group and 645 patients were in the control group. Moreau et al. (2019) studied the efficacy of Dara + bortezomib (V) + thalidomide (T) + dexamethasone (d) vs VTd in NDMM pts (n=1085) in CASSIOPEIA phase III trial. Vorhees et al. reported efficacy of Dara addition to lenalidomide (R), and Vd vs RVd in GRIFFIN study in transplant eligible NDMM patients (n= 207). Dara dose was 16 mg/kg in both studies and the median follow-up was 18.8 months and 22.1 months in CASSIOPEIA and GRIFFIN trial, respectively.
A pooled analysis of these trials showed ORR (OR: 1.73, 95% CI 1.16-2.59; p < 0.008, I2 = 80%). Achievement of MRD negative status was significant in Dara based regimen as compared to control group (OR: 2.47, 95% CI 1.97-3.10; p < 0.00001, I2 = 66%). Dara addition to standard care regimen (Rd and VMP) also decreased the risk of progressive disease (OR: 0.74, 95% CI 0.43-1.28; p < 0.28, I2 = 0%). However, Dara based regimens increased the risk of neutropenia (OR: 3.41, 95% CI 2.68-4.33; p < 0.00001, I2 = 91%), and lymphopenia (OR: 3.43, 95% CI 2.71-4.34; p < 0.0001, I2 = 94%), and pyrexia (OR: 1.42 95% CI 1.11-1.82: p < 0.005, I2=50%) (Figure 1).
Conclusion:
Addition of Dara to the standard care regimen (VRd, VTd) for transplant eligible NDMM achieved the surrogate endpoints with improved efficacy and MRD negative status with manageable toxicity. However, data from more randomized controlled trials are needed.
Anwer:Incyte, Seattle Genetics, Acetylon Pharmaceuticals, AbbVie Pharma, Astellas Pharma, Celegene, Millennium Pharmaceuticals.: Honoraria, Research Funding, Speakers Bureau.

